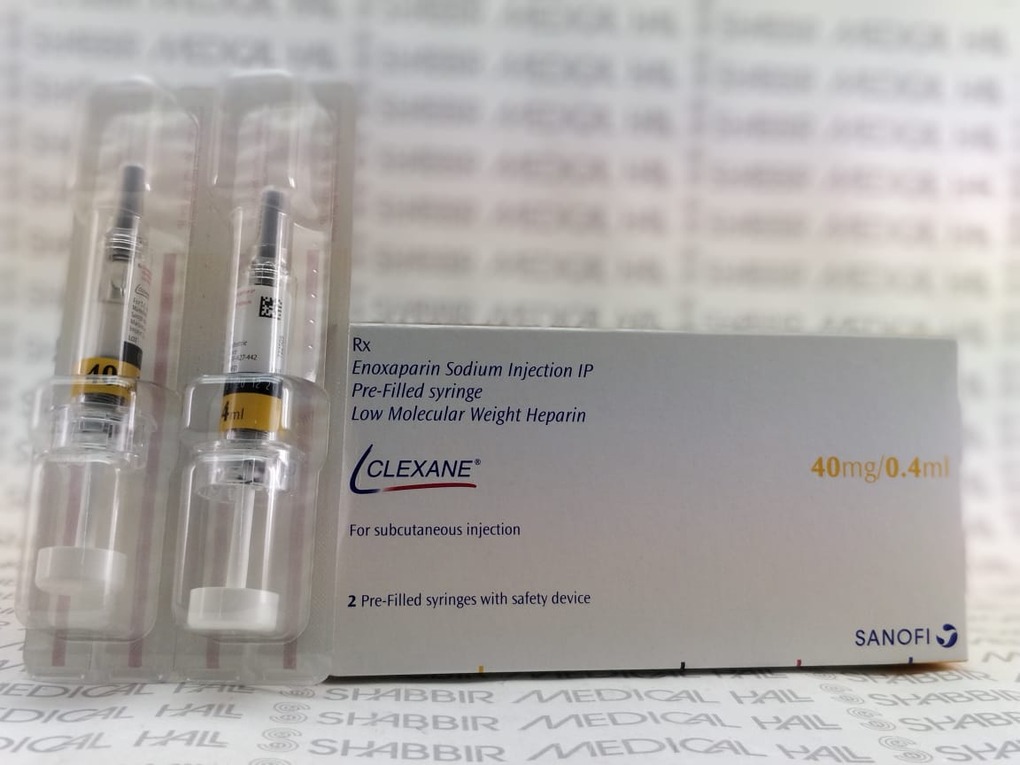
CLEXANE 40MG INJ 0 4ML
Manufactured By SANOFI AVENTIS INDIA LTD
Composition ENOXAPARIN 40MG
RS 376.22
MRP RS 470.27
(20% OFF)
Includes all taxes
Package SIZE
( 0.4ML )
100% Authentic
Products

Free
Shipping*
Products
Return Policy
Description:
Clexane 40mg Injection 0.4ml
(Enoxaparin 40mg) is a low molecular weight heparin (LMWH) anticoagulant manufactured by Sanofi Aventis India Ltd, indicated for the prevention and treatment of deep vein thrombosis (DVT), pulmonary embolism (PE), and thromboembolic complications in a wide range of clinical settings including orthopaedic and general abdominal surgery, acute medical illness with restricted mobility, unstable angina, and non-ST elevation myocardial infarction (NSTEMI). It works by binding to antithrombin III, potently inhibiting Factor Xa and, to a lesser extent, thrombin (Factor IIa), thereby preventing the formation and extension of blood clots in vessels. Available from Shabbir Medical Hall at the best price in India, this genuine prescription injection is available online with fast delivery nationwide.
BENEFITS: Clexane 40mg Injection provides reliable, predictable anticoagulation without the need for routine coagulation monitoring in most patients. As a LMWH, it has a more consistent pharmacokinetic profile than unfractionated heparin, enabling fixed once-daily dosing for prophylaxis. It significantly reduces the incidence of fatal and non-fatal DVT and PE in high-risk surgical and medical patients. In acute coronary syndrome, it reduces the risk of ischaemic events when combined with aspirin. Subcutaneous administration via pre-filled syringe allows convenient self-injection after appropriate patient training.
USAGE OVERVIEW: Clexane 40mg Injection is administered subcutaneously (under the skin), typically in the abdominal wall. For DVT prophylaxis in moderate-to-high risk surgery, the standard dose is 40mg once daily, initiated 12 hours before surgery and continued for 7–10 days or until the patient is fully ambulant. Dosage and duration of therapy must be determined by the prescribing physician based on the clinical indication, patient weight, and renal function.
SAFETY OVERVIEW: The most common side effect is injection site bruising or haematoma. Serious risks include haemorrhage, heparin-induced thrombocytopenia (HIT), hyperkalaemia, and spinal/epidural haematoma when used with neuraxial anaesthesia. Regular platelet count monitoring is recommended during extended therapy. This medicine must only be used under medical supervision with a valid prescription.
Uses / Indications:
• DVT Prophylaxis in Surgery: prevention of venous thromboembolic disease (VTE) in patients undergoing moderate-to-high risk surgery including hip replacement, knee replacement, and abdominal surgery
• DVT Prophylaxis in Medical Patients: prevention of VTE in acutely ill medical patients with severely restricted mobility due to conditions such as heart failure, respiratory failure, sepsis, or acute rheumatic disease
• Treatment of DVT (with or without Pulmonary Embolism): treatment of established deep vein thrombosis, with or without clinically apparent pulmonary embolism, when PE is not haemodynamically unstable
• Acute Coronary Syndromes (NSTEMI/Unstable Angina): prevention of thrombus formation and ischaemic complications in unstable angina and non-Q-wave myocardial infarction (NSTEMI), in combination with oral aspirin
• Acute ST-Elevation Myocardial Infarction (STEMI): adjunct to thrombolytic therapy to prevent re-occlusion
ADDITIONAL USES:
• Prevention of clotting in extracorporeal circulation during haemodialysis
• Extended VTE prophylaxis post-major orthopaedic surgery (up to 5 weeks)
• Bridging anticoagulation in patients on oral anticoagulants
Interactions / Warnings:
SPINAL / EPIDURAL ANAESTHESIA WARNING (BOXED WARNING): USE OF CLEXANE IN PATIENTS RECEIVING NEURAXIAL (SPINAL/EPIDURAL) ANAESTHESIA OR SPINAL PUNCTURE CARRIES A RISK OF SPINAL OR EPIDURAL HAEMATOMA, WHICH CAN RESULT IN LONG-TERM OR PERMANENT PARALYSIS. Ensure at least 12 hours between last prophylactic Clexane dose and epidural/spinal needle insertion; at least 24 hours after therapeutic doses. Do not remove epidural catheter within 12 hours of a Clexane dose. Monitor for signs of spinal haematoma: new back pain, tingling/numbness in lower limbs, bowel/bladder dysfunction.
HAEMORRHAGE RISK: Use with extreme caution in patients with active bleeding, recent surgery (especially neurosurgery, ophthalmological surgery), uncontrolled hypertension, or concomitant use of antiplatelet agents. Protamine sulphate is the antidote for enoxaparin overdose; 1 mg protamine neutralises approximately 1 mg enoxaparin.
RENAL IMPAIRMENT WARNING: Enoxaparin is renally cleared; accumulation occurs in severe renal impairment (CrCl <30 ml/min) — dose reduction to 20mg once daily (prophylaxis) is required; anti-Xa monitoring is strongly recommended.
HEPARIN-INDUCED THROMBOCYTOPENIA (HIT) MONITORING: Monitor platelet count on days 5–7 of therapy and every 2–3 days if therapy continues beyond 7 days. If platelet count drops >50% from baseline or below 100,000/μl — STOP Clexane immediately and test for HIT antibodies.
DRIVING & MACHINERY: No specific restrictions, but underlying condition requiring anticoagulation may affect ability to drive.
ELDERLY (≥65 years): Increased bleeding risk due to age-related reduction in renal function — monitor renal function and consider dose adjustment.
Pregnancy interaction:
• Enoxaparin does NOT cross the placenta and is generally considered the anticoagulant of choice during pregnancy when anticoagulation is clinically indicated (e.g., VTE treatment, antiphospholipid syndrome, mechanical heart valves — specialist guidance required)
• Dose adjustment required during pregnancy due to increased volume of distribution and renal clearance; anti-Xa monitoring is recommended
• Discontinue at least 24 hours before planned delivery or epidural anaesthesia to reduce spinal haematoma risk
• Close haematological and obstetric monitoring is essential throughout pregnancy
BREASTFEEDING:
• Enoxaparin is poorly absorbed orally and is considered compatible with breastfeeding at therapeutic doses
• Consult prescribing physician before continuing Clexane during breastfeeding
CONTRACEPTION WARNING:
• No specific contraceptive requirement; however, pregnancy must be planned in coordination with prescribing physician to ensure safe anticoagulation management at delivery
Expert advice:
1. CORRECT INJECTION TECHNIQUE IS CRITICAL FOR SAFETY AND EFFICACY:
• The subcutaneous injection must be given correctly to ensure adequate absorption and minimise bruising. Counsel patients to: lie flat or sit, pinch a fold of abdominal skin, inject at 45–90° into the fold, never aspirate, and never rub the site afterward. Systematic rotation of injection sites prevents accumulation of haematomas. Patients self-injecting at home should be trained and assessed by a nurse or pharmacist before discharge.
2. NEVER MISS THE SPINAL ANAESTHESIA TIMING WARNING:
• Clexane carries a boxed warning for spinal/epidural haematoma risk. Always ensure patients and their surgical or anaesthetic teams are informed of the most recent Clexane dose before any spinal anaesthesia, epidural insertion or removal, or lumbar puncture. A minimum of 12 hours (prophylactic dose) or 24 hours (therapeutic dose) must elapse before the needle is placed. Failure to observe this timing can result in permanent paralysis.
3. MONITOR RENAL FUNCTION — ENOXAPARIN ACCUMULATES IN RENAL IMPAIRMENT:
• Enoxaparin is cleared by the kidneys. In patients with severe renal impairment (CrCl <30 ml/min), standard dosing leads to dangerous drug accumulation and serious haemorrhagic risk. For DVT prophylaxis, the dose must be reduced to 20mg once daily; anti-Xa monitoring is strongly recommended. Always check serum creatinine/CrCl before dispensing Clexane in elderly or diabetic patients.
4. WATCH FOR HIT — A PARADOXICAL AND LIFE-THREATENING REACTION:
• Although the incidence of HIT Type II is lower with LMWH than unfractionated heparin, it remains a serious risk. Paradoxically, HIT causes thrombosis despite the platelet count falling. Check platelet counts on days 5–7 and every 2–3 days thereafter in extended-use patients. If platelet count drops by more than 50% from baseline, stop Clexane immediately and arrange urgent haematologist review.
5. COUNSEL PATIENTS ON BLEEDING SIGNS AND WHEN TO SEEK EMERGENCY CARE:
• All patients on Clexane must be counselled to seek immediate medical attention for: unexpected or severe bruising, blood in urine or stools, vomiting blood, prolonged bleeding from cuts, sudden severe headache, back pain with leg weakness or numbness (spinal haematoma). A medication alert card listing Clexane use and emergency contacts is highly recommended.
MONITORING ADVICE:
• Platelet count (CBC): Baseline; days 5–7; every 2–3 days on extended therapy
• Serum creatinine / CrCl: Baseline, especially in elderly patients and those with diabetes or hypertension
• Anti-Xa levels: Required in renal impairment, pregnancy, extreme body weight (<45 kg or >100 kg)
• Signs of bleeding: Daily clinical assessment during in-hospital therapy; patient self-monitoring on discharge
• Liver function tests (ALT/AST): Periodic monitoring during extended therapy
COMPLIANCE TIPS:
• Set a daily alarm for the same time — once-daily dosing for DVT prophylaxis must be consistent
• Use a sharps disposal bin for safe disposal of used pre-filled syringes at home
• Rotate injection sites — keep a simple diagram to track sites used
• Carry a medication alert card identifying Clexane use for all emergency and surgical consultations
• Store pre-filled syringes below 25°C and never freeze them — freezing destroys the drug
SAFETY TIPS:
• Do NOT use if the solution is cloudy, coloured, or contains particles
• Inform all treating doctors, dentists, and surgeons that you are on Clexane before any invasive procedure
• Avoid contact sports or activities with high risk of injury while on anticoagulation
• Do not use over-the-counter NSAIDs (ibuprofen, diclofenac) without physician approval — they increase bleeding risk
Side Effects:
• Injection site reactions: bruising, haematoma, pain, erythema, and nodules at injection site
• Haemorrhage (bleeding): minor bleeding from wounds, gums, or nose
• Elevated liver enzymes (ALT, AST) — usually asymptomatic and reversible
• Anaemia (in some patients on long-term therapy)
• Thrombocytopenia (mild, Type I — transient and benign)
SERIOUS SIDE EFFECTS (contact your doctor immediately):
• Major Haemorrhage: spinal/epidural haematoma (can cause permanent paralysis — see spinal anaesthesia warning), intracranial haemorrhage, gastrointestinal bleeding, retroperitoneal haematoma — seek emergency care
• Heparin-Induced Thrombocytopenia (HIT Type II): immune-mediated platelet drop with paradoxical thrombosis risk — discontinue Clexane immediately if HIT is suspected; requires urgent haematologist review
• Hyperkalaemia: enoxaparin can suppress aldosterone production, causing dangerous rises in serum potassium — particularly in patients with renal impairment, diabetes, or those on ACE inhibitors/ARBs/potassium-sparing diuretics
• Skin necrosis at injection site: rare but serious; associated with HIT
• Severe allergic reactions (anaphylaxis, urticaria, angioedema): seek emergency care
EMERGENCY SIGNS — SEEK IMMEDIATE MEDICAL HELP:
• Sudden severe back pain, leg weakness or numbness (spinal haematoma)
• Signs of serious bleeding: vomiting/coughing blood, blood in urine or stools, sudden severe headache
• Signs of HIT: new clots forming while on treatment, skin changes at injection site
How to use:
• DVT Prophylaxis (Moderate-High Risk Surgery): 40mg ONCE DAILY subcutaneously; start 12 hours BEFORE surgery; continue for 7–10 days post-surgery (up to 5 weeks for hip replacement)
• DVT Prophylaxis (Medical Patients): 40mg ONCE DAILY subcutaneously for 6–14 days
• Treatment of DVT/PE: 1.5 mg/kg ONCE DAILY or 1 mg/kg TWICE DAILY subcutaneously; continue for at least 5 days and until therapeutic oral anticoagulation (INR 2–3) is established
• Unstable Angina/NSTEMI: 1 mg/kg every 12 hours subcutaneously (with aspirin); continue for 2–8 days
• Renal Impairment: dose reduction required for patients with CrCl <30 ml/min — consult physician
ROUTE OF ADMINISTRATION:
• Subcutaneous (SC) injection — administered under the skin in the anterolateral or posterolateral abdominal wall (alternate injection sites)
• DO NOT administer by intramuscular (IM) injection
• DO NOT use the pre-filled syringe if the solution is not clear, colourless or pale yellow, or if particulate matter is present
INJECTION TECHNIQUE:
• Lie down or sit comfortably; pinch a skin fold between thumb and forefinger
• Insert the full needle length at 45–90° angle; do not aspirate; inject entire contents slowly
• Do not rub the injection site after administration — this may cause bruising
• Rotate injection sites systematically
MISSED DOSE:
• Inject as soon as remembered, unless it is almost time for the next dose
• Never double the dose
STORAGE:
• Store below 25°C; do not freeze
• Keep in original packaging to protect from light
• Keep out of reach of children
• Do not use after the expiry date printed on the label
How it works:
MECHANISM OF ACTION:
Enoxaparin exerts its anticoagulant effect primarily through binding to antithrombin III (AT-III), a natural coagulation inhibitor. This binding produces conformational changes in AT-III that markedly accelerate its inhibitory action on:
• Factor Xa (primary target): inhibition of Factor Xa prevents the conversion of prothrombin to thrombin, blocking the final common pathway of coagulation → prevents new clot formation
• Factor IIa (thrombin): moderate inhibition reduces thrombin-mediated fibrinogen conversion to fibrin
• Anti-Xa : Anti-IIa ratio for enoxaparin is approximately 3.8:1, giving it more selective anti-Xa activity compared to unfractionated heparin
NET RESULT:
Inhibition of coagulation cascade → prevention of thrombus formation and extension → reduced risk of DVT, PE, and arterial thrombosis.
KEY ADVANTAGES:
• Predictable, weight-based pharmacokinetics — no routine aPTT monitoring required in most patients
• Subcutaneous once-daily dosing for prophylaxis — convenient and patient-friendly
• Lower risk of heparin-induced thrombocytopenia (HIT) compared to unfractionated heparin
• Clinically validated across surgical prophylaxis, medical DVT prevention, and ACS management
Faq for medicine:
Clexane 40mg contains Enoxaparin, a low molecular weight heparin used to prevent deep vein thrombosis and pulmonary embolism in hospitalized medical or surgical patients, treat acute DVT and PE, and prevent ischemic complications in unstable angina and NSTEMI. Clexane inhibits Factor Xa and thrombin, providing predictable anticoagulation without the need for routine coagulation monitoring.
2.How should Clexane 40mg injection be administered subcutaneously?
Clexane 40mg is injected subcutaneously into the anterolateral or posterolateral abdominal wall, alternating sides with each dose. Insert the needle perpendicularly into a pinched skin fold without expelling the air bubble beforehand. Do not massage the injection site after administration, as this can cause bruising. Clexane should be stored at room temperature below 30°C and protected from light.
3.What is the correct Clexane 40mg dose for medical patients at VTE risk?
For thromboprophylaxis in hospitalized medical patients with restricted mobility, Clexane 40mg once daily subcutaneously is the standard dose, typically for 6–14 days or until mobility is restored. For surgical prophylaxis, the first dose is given 2 or 12 hours before the procedure. For hip replacement, extended prophylaxis for up to 35 days post-surgery may be recommended.
4.Can Clexane 40mg be used safely in patients with kidney impairment?
Clexane 40mg should be used with caution in renal impairment. In severe CKD (CrCl <30mL/min), Enoxaparin accumulates and standard doses may cause excessive anticoagulation. Dose reduction to 20mg once daily for prophylaxis is recommended in severe renal impairment. Anti-Xa level monitoring is advised in renally impaired patients to ensure safe and therapeutic Clexane exposure.
5.What are the signs of Clexane 40mg overdose or excessive anticoagulation?
Signs of Clexane 40mg overdose include excessive bruising, prolonged bleeding from cuts, blood in urine or stools, unusual headache, joint swelling, and spinal bleeding in neuraxial anesthesia patients. Protamine sulfate partially reverses Enoxaparin, neutralizing approximately 60% of anti-Xa activity. Serious bleeding with Clexane requires emergency medical intervention and immediate discontinuation of Enoxaparin.
6.Does Clexane 40mg require INR monitoring like warfarin?
No, Clexane 40mg does not require routine INR monitoring. Its anticoagulant effect can be assessed using anti-Xa levels when clinically needed, such as in morbidly obese patients, pregnant women, or those with renal impairment. Unlike warfarin, Clexane has predictable pharmacokinetics, fixed-dose administration, and no dietary interactions, making it more convenient for short-term anticoagulation in hospitalized patients.
Medicine interaction:
• Antiplatelet agents (aspirin, clopidogrel, prasugrel, ticagrelor, NSAIDs, dipyridamole): combination increases haemorrhagic risk — use only when clinically indicated; monitor closely for bleeding signs
• Oral anticoagulants (warfarin, acenocoumarol): concurrent use increases anticoagulant effect; overlap periods during bridging therapy require careful INR monitoring
• Thrombolytics (streptokinase, alteplase, tenecteplase): risk of serious haemorrhage when combined; use only under strict specialist supervision
• Dextran: additive anticoagulant and antiplatelet effect — increased bleeding risk
• Systemic corticosteroids: may increase risk of GI bleeding (additive mucosal injury)
• ACE inhibitors, ARBs, potassium-sparing diuretics, potassium supplements: additive risk of hyperkalaemia — monitor serum potassium levels closely
VACCINE INTERACTIONS:
• No specific vaccine interactions documented for enoxaparin
SUPPLEMENT INTERACTIONS:
• Omega-3 fatty acids / fish oil supplements: mild antiplatelet effect may increase bleeding risk
• Vitamin E (high dose): antiplatelet properties; monitor for increased bruising
• Herbal products (ginkgo biloba, garlic, ginger, ginseng, turmeric — high dose): antiplatelet/anticoagulant properties; inform your physician