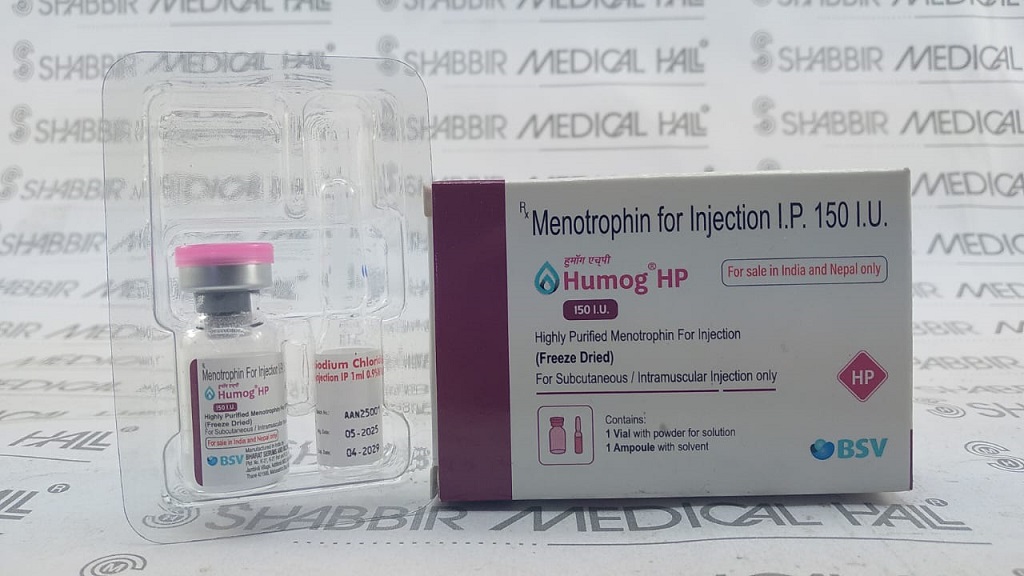
Humog 150 HP Injection
![]() Item requires a valid prescription
Item requires a valid prescription
Manufactured By Bharat Serums Vaccines Limited
Composition Menotrophin 150IU
RS 1777.01
MRP RS 2538.58
(30% OFF)
Includes all taxes
Package SIZE
( 1 Injection in 1 vial )
100% Authentic
Products

Free
Shipping*
Products
Return Policy
Description:
Humog 150 HP Injection (Menotrophin 150 IU) is a Highly Purified human Menopausal Gonadotropin (hMG-HP) manufactured by Bharat Serums & Vaccines Limited (BSV), containing a 1:1 ratio of Follicle-Stimulating Hormone (FSH 75 IU) and Luteinizing Hormone (LH 75 IU) derived from the urine of postmenopausal women. It is indicated for controlled ovarian stimulation (COS) in women undergoing assisted reproductive technology (ART) procedures such as IVF, ICSI, and IUI, as well as for the treatment of anovulatory infertility in women with PCOS or unexplained infertility, and for male hypogonadotropic hypogonadism. Available from Shabbir Medical Hall at the best price in India, this genuine prescription injection is available online with fast delivery nationwide.
BENEFITS: Humog 150 HP provides a physiologically balanced combination of FSH and LH activity in a highly purified urinary formulation. FSH drives follicular growth and maturation in the ovaries, while LH supports follicular development and oestrogen production. The dual-hormone action closely mimics the natural mid-cycle hormonal surge, optimising follicle recruitment and egg quality for ART procedures. For male patients, LH stimulates Leydig cells to produce testosterone, supporting spermatogenesis. Clinical evidence supports hMG-HP's effectiveness in achieving high-quality oocyte yields comparable to recombinant FSH, with the added benefit of intrinsic LH activity without supplementation.
USAGE OVERVIEW: Humog 150 HP is administered as a subcutaneous (SC) or intramuscular (IM) injection under strict medical supervision by a fertility specialist or reproductive endocrinologist. The standard starting dose is 150 IU daily (1 vial), adjusted based on individual ovarian response monitored by transvaginal ultrasound and serum oestradiol levels. Treatment cycles typically span 7–12 days depending on follicular response, always followed by a trigger injection (hCG) to finalise egg maturation.
SAFETY OVERVIEW: The most common side effects include injection site reactions, headache, nausea, and abdominal bloating. The most serious risk is Ovarian Hyperstimulation Syndrome (OHSS) — a potentially life-threatening condition requiring immediate medical attention. Multiple pregnancy risk is significantly increased. This medicine must be administered only under specialist supervision with regular monitoring.
Uses / Indications:
• Controlled Ovarian Stimulation (COS) for ART: IVF (In Vitro Fertilisation), ICSI (Intracytoplasmic Sperm Injection), IUI (Intrauterine Insemination) — to stimulate development of multiple mature follicles
• Anovulatory Infertility: Treatment of women who fail to ovulate due to hormonal dysfunction (hypothalamic or pituitary origin), including WHO Group I and Group II anovulation
• Polycystic Ovary Syndrome (PCOS): Ovarian stimulation in PCOS patients with clomiphene-resistant anovulatory infertility
• Unexplained Infertility: Superovulation induction in conjunction with IUI
PRIMARY USES (MEN):
• Hypogonadotropic Hypogonadism: Treatment of male infertility secondary to insufficient pituitary gonadotropin secretion, resulting in low testosterone and impaired spermatogenesis
• Low Sperm Count (Oligospermia): In combination with hCG, to stimulate sperm production in men with gonadotropin deficiency
• Delayed Puberty (Male): Where hypogonadotropic hypogonadism is confirmed
ADDITIONAL USES:
• Superovulation in donor egg programmes and oocyte cryopreservation cycles
• Fertility preservation stimulation before chemotherapy or radiation therapy (under specialist guidance)
Interactions / Warnings:
OHSS RISK STRATIFICATION & PREVENTION: HIGH-RISK PATIENTS requiring enhanced monitoring: Young women (<35 yrs), low BMI, polycystic ovaries (PCO morphology on ultrasound), prior OHSS history, antral follicle count >20, serum AMH >3.5 ng/mL, oestradiol >3,000 pg/mL on trigger day. PREVENTION STRATEGIES: GnRH antagonist protocols with GnRH agonist trigger (instead of hCG) for freeze-all cycles; coasting (withholding gonadotropins when E2 rises rapidly); low-dose hCG trigger; elective embryo cryopreservation (freeze-all) with deferred frozen embryo transfer. CABERGOLINE: May be prescribed to prevent moderate OHSS — follow specialist prescription.
MULTIPLE PREGNANCY WARNING: The probability of multiple gestations in IVF is managed primarily by number of embryos transferred (single embryo transfer / SET policy). In IUI or anovulation cycles, if >3 follicles ≥14 mm develop, the cycle may be cancelled or converted to IVF to avoid high-order multiple risk — follow clinic policy strictly.
OVARIAN TORSION: Enlarged ovaries (>5 cm) during stimulation increase torsion risk — avoid strenuous exercise, sexual intercourse, and sudden positional changes during stimulation and for several days post-retrieval.
THROMBOEMBOLISM WARNING: Women with personal or family history of thrombosis, antiphospholipid syndrome, Factor V Leiden, or protein C/S deficiency require haematology review before ART — LMWH prophylaxis is commonly prescribed.
PRE-TREATMENT SCREENING (MANDATORY): Gynaecological evaluation: Transvaginal ultrasound (antral follicle count, ovarian morphology, uterine assessment) — confirm absence of ovarian cysts, fibroids, or uterine anomalies before starting. Hormonal baseline: Serum FSH, LH, oestradiol, AMH, TSH, prolactin — on cycle day 2–3. Partner semen analysis: Before commencing any ovarian stimulation cycle. Infectious disease screening: HBsAg, anti-HCV, HIV, VDRL — required before ART procedures. Exclude primary ovarian insufficiency, thyroid dysfunction, and hyperprolactinaemia before commencing gonadotropin therapy.
Pregnancy interaction:
• Humog 150 HP is used specifically to assist conception — once pregnancy is confirmed, STOP Menotrophin immediately unless specifically instructed otherwise by your fertility specialist.
• If pregnancy occurs during treatment, there is a significantly increased risk of MULTIPLE GESTATION (twins, triplets, higher-order multiples) — associated with higher rates of premature birth, low birth weight, and maternal obstetric complications.
• Ectopic pregnancy risk is elevated in women with a history of tubal disease or prior ectopic pregnancy; early ultrasound confirmation of intrauterine pregnancy location is essential.
• Menotrophin has NOT been shown to be teratogenic in correctly monitored treatment; however, inadvertent exposure in early undetected pregnancy should be discussed with the fertility specialist.
BREASTFEEDING:
• Humog 150 HP is not indicated during breastfeeding. If conception occurs during lactation-suppressed fertility treatment, breastfeeding should be discontinued and specialist guidance sought.
CONTRACEPTION WARNING:
• Patients must not use contraceptives during fertility treatment cycles. All sexual activity during stimulation and following hCG trigger must follow fertility clinic guidance to optimise conception timing or avoid unexpected multiple fertilisation in non-ART cycles.
Expert advice:
1. NEVER SELF-ADMINISTER WITHOUT TRAINING:
• Humog 150 HP Injection must be prescribed and initially administered under direct medical supervision. If your fertility clinic approves self-administration (SC route), ensure you receive complete injection technique training from the clinic nurse — including reconstitution, air bubble removal, site rotation, and safe sharps disposal. Incorrect administration can reduce efficacy and increase complication risk.
2. RECONSTITUTE CORRECTLY — ADMINISTER IMMEDIATELY:
• Humog 150 HP is supplied as a lyophilised (freeze-dried) powder. Add the provided diluent (sterile water for injection) slowly into the vial and gently swirl (do not shake) until fully dissolved. Use the reconstituted solution within 30 minutes. NEVER use if the solution is cloudy, discoloured, or contains particles.
3. MONITOR YOUR RESPONSE CLOSELY — ATTEND ALL SCANS:
• Ovarian response to Menotrophin is highly individual. Attending every scheduled transvaginal ultrasound scan (every 2–3 days during stimulation) is non-negotiable. Scans assess follicle count and size, and oestradiol levels guide dose adjustments. Missing a scan may lead to either under-stimulation (cycle cancellation) or dangerous over-response (OHSS).
4. KNOW THE OHSS WARNING SIGNS — ACT IMMEDIATELY:
• Ovarian Hyperstimulation Syndrome is the most serious risk of gonadotropin therapy. Contact your fertility clinic immediately if you experience: rapid weight gain (>1 kg in 24 hours), severe abdominal distension and pain, difficulty breathing, persistent nausea/vomiting, or greatly reduced urine output. Do NOT wait — severe OHSS requires hospitalisation and can be life-threatening.
5. DO NOT ADJUST YOUR OWN DOSE:
• Never increase or decrease the number of vials per injection without explicit instruction from your fertility specialist. Over-stimulation from unsupervised dose escalation is the leading preventable cause of severe OHSS. Your dose is reviewed at every monitoring visit based on real-time scan and blood test data.
MONITORING ADVICE:
• Baseline: Transvaginal ultrasound (antral follicle count, uterine assessment) + serum FSH, LH, E2, AMH before cycle start
• Stimulation monitoring: Transvaginal ultrasound + serum oestradiol every 2–3 days from day 5–6 of stimulation
• Trigger criteria: Lead follicle(s) ≥18 mm diameter; ≥3 follicles ≥17 mm in IVF
• Post-trigger: Egg collection 34–36 hours after hCG; luteal phase support commenced immediately
• Pregnancy test: Serum βhCG — 14 days after egg collection/embryo transfer; early viability scan at 6–7 weeks
COMPLIANCE TIPS:
• Administer injections at the same time each day — consistency in timing is critical for hormonal synchrony
• Store unopened vials in the refrigerator (2–8°C) — never in the freezer, never at room temperature for prolonged periods
• Rotate injection sites each day to prevent subcutaneous fibrosis and improve absorption
• Keep a daily stimulation diary: vial batch number, injection time, site used, any symptoms — bring to every monitoring appointment
• Carry your fertility specialist's contact number at all times during stimulation
SAFETY TIPS:
• Avoid strenuous exercise, heavy lifting, and high-impact activity during stimulation and for 1–2 weeks post egg collection — enlarged ovaries are at increased torsion risk
• Avoid alcohol during fertility treatment — alcohol reduces oocyte quality and implantation rates
• Inform your dentist, GP, and any other treating physician that you are currently undergoing IVF stimulation with gonadotropins
• Do NOT take any over-the-counter NSAIDs (ibuprofen, aspirin) without fertility clinic approval — some protocols restrict these near trigger and retrieval
• Women with PCOS: Inform your fertility specialist if you have ever had OHSS in a prior cycle — preventive protocol modification (GnRH antagonist + agonist trigger / freeze-all strategy) significantly reduces repeat OHSS risk
Side Effects:
• Injection site reactions: Pain, redness, swelling, bruising at the injection site — rotate sites to minimise
• Headache — usually mild and transient
• Nausea, vomiting, stomach discomfort / abdominal bloating
• Breast tenderness (women) — due to rising oestradiol levels
• Pelvic discomfort / lower abdominal pain — associated with follicular growth
• Mood changes, irritability, fatigue — hormonal fluctuations during stimulation
• Mild ovarian enlargement — monitored routinely by ultrasound
SERIOUS SIDE EFFECTS — OVARIAN HYPERSTIMULATION SYNDROME (OHSS):
STOP INJECTIONS AND CONTACT YOUR FERTILITY CLINIC IMMEDIATELY if you experience:
• Mild OHSS: Abdominal bloating, mild pain, slight ovarian enlargement — usually resolves with rest
• Moderate OHSS: Significant abdominal distension, nausea, vomiting, diarrhoea, reduced urine output, ovarian enlargement
• Severe OHSS (MEDICAL EMERGENCY): Rapid weight gain (>1 kg/day), severe abdominal pain and distension, difficulty breathing (pleural effusion/ascites), very reduced urine output, dizziness/fainting — REQUIRES IMMEDIATE HOSPITALISATION
OTHER SERIOUS EFFECTS:
• Multiple Pregnancy: Risk of twins, triplets, or higher-order multiples is significantly elevated — associated with increased obstetric and neonatal risks
• Ectopic Pregnancy: Slightly increased risk in women with pre-existing tubal pathology
• Thromboembolic Events (rare): Deep vein thrombosis (DVT), pulmonary embolism — associated with OHSS and high oestradiol levels; seek immediate care if leg pain/swelling or chest pain/breathlessness occurs
• Ovarian Torsion (rare): Sudden severe one-sided pelvic pain requiring emergency evaluation
EMERGENCY SIGNS — SEEK IMMEDIATE MEDICAL HELP:
• Sudden severe abdominal pain with rapid weight gain and difficulty breathing (severe OHSS)
• Chest pain or one-sided leg pain and swelling (thromboembolism)
• Sudden one-sided pelvic pain (possible ovarian torsion)
How to use:
WOMEN – CONTROLLED OVARIAN STIMULATION (IVF/ICSI):
• Starting dose: 150–225 IU (1–1.5 vials) subcutaneously (SC) or intramuscularly (IM) ONCE DAILY
• Dose adjustments: Based on ovarian response assessed by transvaginal ultrasound (follicle size/count) and serum oestradiol every 2–3 days
• Stimulation phase: Typically 7–12 days until lead follicle(s) reach ≥18 mm diameter
• Trigger: Once adequate follicular development is confirmed, an hCG injection (5,000–10,000 IU) or recombinant LH is administered 34–36 hours before egg collection
WOMEN – ANOVULATORY INFERTILITY / IUI:
• Starting dose: 75–150 IU SC/IM daily
• Monitoring: Transvaginal ultrasound every 2–3 days; dose adjusted to mono-follicular development to minimise multiple pregnancy risk
• Trigger: hCG when lead follicle ≥18 mm; IUI performed 36–40 hours post-trigger
MEN – HYPOGONADOTROPIC HYPOGONADISM:
• Pre-treatment: hCG injections (1,500–5,000 IU, 2–3x/week) for 4–6 months until testosterone normalises
• Then add Humog 150 HP: 75–150 IU IM/SC 2–3x/week alongside continued hCG
• Duration: Up to 18 months or until adequate sperm count achieved
ROUTE OF ADMINISTRATION:
• SC (subcutaneous — preferred for self-administration): Abdomen, upper thigh, or upper arm
• IM (intramuscular): Outer thigh or gluteal region — usually clinic-administered
• Reconstitute lyophilised powder with provided diluent immediately before use; administer within 30 minutes of reconstitution; rotate injection sites
STORAGE:
• Store at 2–8°C (refrigerator) — do NOT freeze
• Keep in original packaging; protect from light
• Once reconstituted: use immediately; discard unused portion
• Keep out of reach of children; do not use after expiry date
How it works:
FSH (FOLLICLE-STIMULATING HORMONE) ACTION:
• Binds to FSH receptors on granulosa cells in ovarian follicles
• Stimulates follicular growth, proliferation of granulosa cells, and maturation of multiple follicles simultaneously
• Induces aromatase enzyme activity — converting androgens to oestradiol (oestrogen), which supports endometrial growth and signals pituitary feedback
• Promotes expression of LH receptors on granulosa cells in preparation for the LH surge
LH (LUTEINIZING HORMONE) ACTION:
• Binds to LH/hCG receptors on theca cells surrounding follicles
• Stimulates production of androgen precursors (androstenedione, testosterone) in theca cells, which are then aromatised by granulosa cells to oestradiol
• In men: acts on testicular Leydig cells to stimulate testosterone synthesis and supports spermatogenesis
SYNERGISTIC DUAL HORMONE EFFECT:
• The FSH + LH combination in Humog 150 HP closely replicates the natural endogenous gonadotropin pattern
• This dual action optimises both follicle number and oocyte quality compared to FSH-only protocols for certain patient subgroups
• Following adequate follicular development, an hCG trigger injection is administered to mimic the natural LH surge, completing egg maturation (final oocyte maturation / ovulation trigger)
IN MEN:
• FSH + LH together stimulate the testicular germinal epithelium and Leydig cells, restoring testosterone production and spermatogenesis in hypogonadotropic hypogonadism patients
Faq for medicine:
Humog 150 HP Injection contains Menotrophin (HMG), a combination of FSH and LH derived from human urine. It stimulates ovarian follicle development in women, triggering egg release from the ovary. It is used for ovulation induction and in ART protocols. Humog helps restore hormonal balance needed for successful conception in infertile women.
2.Can Humog 150 HP Injection be used to treat male infertility?
Yes, Humog 150 HP Injection is used in men to treat hypogonadotropic hypogonadism, low sperm count, and male infertility. Its LH component stimulates testosterone production, while FSH supports spermatogenesis. Humog is administered under endocrinologist supervision and is typically combined with hCG therapy for optimal results in restoring male reproductive function.
3.What is Menotrophin in Humog 150 HP Injection and how does it work?
Menotrophin in Humog 150 HP Injection is a highly purified mixture of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) extracted from human menopausal urine. FSH promotes follicular growth and sperm production, while LH triggers ovulation and supports testosterone synthesis. This dual hormonal action makes Humog effective for both male and female fertility issues.
4.What precautions should be taken before using Humog 150 HP Injection?
Before using Humog 150 HP Injection, patients must undergo a complete fertility workup including hormonal profiling and ultrasound. It is contraindicated in primary ovarian failure, uncontrolled thyroid or adrenal disorders, and hormone-sensitive tumors. Medical supervision with cycle monitoring is mandatory. Women with PCOS require especially careful dose management to prevent ovarian hyperstimulation.
5.What are the common side effects of Humog 150 HP Injection?
Common side effects of Humog 150 HP Injection include injection site reactions such as pain, redness, and swelling. Women may experience abdominal discomfort, bloating, or mild pelvic pain due to follicular stimulation. Ovarian hyperstimulation syndrome (OHSS) is a serious risk. Multiple pregnancies can also occur. Men may notice gynecomastia or acne during therapy.
6.How does Humog 150 HP Injection differ from Lupi-FSH in fertility treatment?
Humog 150 HP Injection contains both FSH and LH (Menotrophin), whereas Lupi-FSH contains only FSH (Urofollitropin). Humog is suitable for patients requiring combined gonadotropin support, particularly those with low LH levels. Lupi-FSH is preferred when isolated FSH stimulation is needed. The choice depends on the patient's hormonal profile and treatment protocol.
Medicine interaction:
• hCG (Human Chorionic Gonadotropin): Used intentionally as the ovulation trigger after Humog stimulation — timing is precisely protocol-driven; do not self-administer hCG without specialist instruction
• GnRH Agonists (Leuprolide, Buserelin, Nafarelin): Co-administered in long and short GnRH-agonist IVF protocols to suppress premature LH surge; Humog stimulation begins after pituitary downregulation is confirmed
• GnRH Antagonists (Cetrorelix, Ganirelix): Co-administered in antagonist IVF protocols to prevent premature ovulation; added on day 5–6 of stimulation when lead follicle reaches ~14 mm
• Clomiphene Citrate: May be used in sequential protocols; do not combine without specialist guidance
• Progesterone / Luteal Phase Support: Prescribed after egg collection (IVF/ICSI) or after IUI to support implantation — commonly progesterone vaginal pessaries, IM injections, or oral dydrogesterone
• Insulin / Metformin (PCOS patients): Metformin may be continued through stimulation to reduce OHSS risk in PCOS — confirm continuation with fertility specialist
• Anticoagulants (Aspirin, LMWH/Heparin): Low-dose aspirin or LMWH may be prescribed concurrently to reduce thromboembolic risk in high-responders or OHSS prevention protocols — follow specialist prescription only
VACCINE INTERACTIONS:
• Diagnostic Interference — Gonadotropin assays (serum FSH, LH): Humog administration will elevate measured gonadotropin levels — inform all treating physicians that you are on Menotrophin before any hormonal blood test
SUPPLEMENT INTERACTIONS:
• DHEA, CoQ10: Widely used as adjunct fertility supplements — inform fertility specialist of all supplements being taken
• Vitamin D, Folic Acid: Generally safe and recommended periconceptionally — continue as directed
• Herbal supplements: Do NOT use any herbal fertility remedies (Vitex/Chasteberry, Dong Quai, Red Clover) concurrently — interactions with gonadotropin response are unpredictable